History of Randomized Clinical Trials in Ovarian Cancer: Pre-Taxol Era
For many years (from the early 60s to late 70s), the "standard" ovarian cancer chemotherapy was single agent melphalan (or chemotherapy with a related "alkylating agent," such as cyclophosphamide). These "alkylators" were inexpensive and usually well tolerated oral drugs. In the late 70s, the NCI reported the results of a randomized clinical trial in the New England Journal of Medicine in which a complex and toxic combination ("HEXA-CAF") ostensibly produced superior results, compared to single agent melphalan. But this study was not confirmed. By the early 80s, some data appeared initially to support the concept that cisplatin-based combinations might produce superior outcomes. The new standard became cisplatin + cyclophosphamide (CTX). Later on, carboplatin was introduced, and the combination of carboplatin + CTX was found to produce results equivalent to cisplatin + CTX, but the former combination was better tolerated. This became the new standard. However, a landmark meta-analysis published in the early 90s, analyzing studies including 8,000 patients and 6,000 deaths to determine what had been learned about optimum first line chemotherapy concluded that "no conclusions could be made." The study authors concluded that previous studies (often involving hundreds of patients) had been much too small to provide statistical power, and the authors announced that their cooperative group was initiating a prospective trial to compare single agent carboplatin versus the combination of cisplatin + doxorubicin + CTX which was to accrue 2,500 patients.
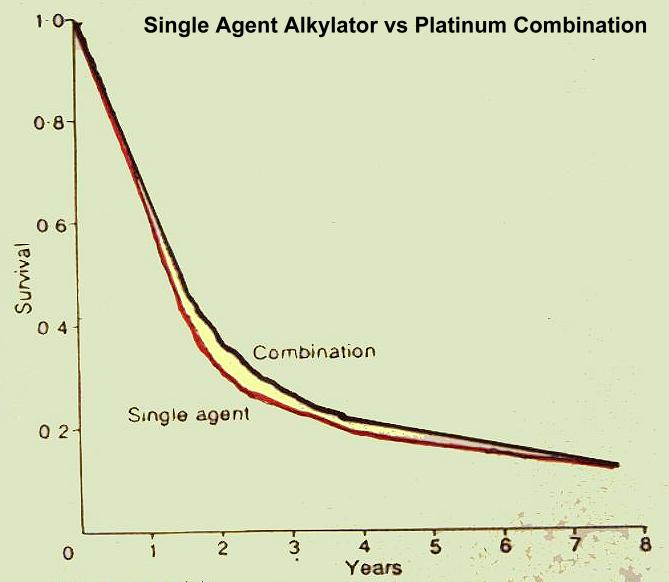
It is very important to note that it is widely accepted that platinum-based combination chemotherapy has been proven to be superior to single agent alkylating agent therapy (used in ovarian cancer since the 1960s). However, this is not true, as clearly shown in the landmark meta-analysis, as shown by the survival curves (p = 0.23). A re-analysis of the original meta-analysis still did not show any advantage, 10 years out, for platinum-based therapy over single agent alkylator therapy. In other words it has NOT been shown that platinum-based combination therapy is superior to single agent alkylator therapy. Yet many would maintain that not to treat an ovarian cancer patient with platinum is tantamount to malpractice. This position cannot be supported (and is, in fact, refuted) by prospective, randomized clinical trials.
Taxol Bursts Upon the Ovarian Cancer Scene
Midway into the above 2,500 patient study, the glamour drug of the 1990s, paclitaxel (Taxol), came along. A prospective, randomized trial showed the superiority of cisplatin/Taxol over carboplatin/cyclophosphamide, and the former combination quickly became the new standard, which ostensibly made the ongoing, long-term, expensive study of cisplatin + doxorubicin + CTX instantly irrelevant and obsolete. The new cisplatin/Taxol combination was, parenthetically, vastly more expensive and toxic than was the oral melphalan "standard" of the 1970s (>$25,000 per patient, as opposed to <$1,000 per patient). And does Taxol add anything to cisplatin (or carboplatin) alone? Of the drugs introduced in the 1990s, probably no drug was more highly touted than Taxol, and in no disease was it more highly touted than in ovarian cancer. Indeed, it would be accurate to state that most clinical oncologists probably feel that it would be tantamount to malpractice not to use either Taxol/cisplatin or Taxol/carboplatin as first line therapy in ovarian cancer. This point of view was, in fact, given the imprimatur of the NCI's authoritative PDQ description of state of the art therapy.
Flies in the Taxol Ointment
A recent, large, multi-institutional trial (Gynecologic Oncology Group # 132) randomized ovarian cancer patients to (1) Taxol/cisplatin, (2) Taxol alone, and (3) cisplatin alone. Patients could be crossed over to the other drugs in the event of disease progression. The result? Taxol alone was inferior to the other two regimens, while cisplatin alone was, if anything, superior to the Taxol/cisplatin combination in complete remission rate and duration of response and most certainly was no worse than the combination. So what is the level of evidence supporting the use of Taxol/cisplatin over cisplatin alone? And given that carboplatin has been shown (in combination trials) to be therapeutically equivalent to cisplatin, but less toxic, is it not reasonable to consider using single agent carboplatin alone, as first line chemotherapy?
In a very recent editorial (JNCI 92:674-5,2000), Dr. William McGuire succinctly summarized the status of clinical trials in ovarian cancer and presented his own view of the future, stating "thus, even though more than 5400 patients with advanced ovarian cancer have been accrued to randomized trials in the last decade to "fine tune" the regimen with the best therapeutic index, what is best is still unclear." McGuire further maintained that randomized clinical trials must now be international in scope, as single institutions do not have the capability to carry out studies of sufficient statistical power, nor even do individual cooperative groups, nor do intergroup studies combining several cooperative groups; rather only a truly global effort is up to the task of methodically testing all of the myriad potential combinations to define the next 2 month improvement in median survival, based on the paradigm of one size fits all chemotherapy.
By coincidence, in a perfect example of just such a global effort, the results of a very important large international study were presented at the American Society of Clinical Oncology annual meeting in New Orleans, May 20, 2000. The Third International Collaborative Ovarian Neoplasm Study (ICON3) included 2074 patients from 132 hospitals in 8 countries. At the time of this second planned analysis, median follow up was 29 months, 925 patients remained alive without progressive disease and 1293 had either died or developed progressive disease. Two year survival was 64% in the group treated with carboplatin/Taxol (now considered "mandatory" standard therapy in the USA) and an identical 64% in patients treated either with single agent carboplatin or with the very old regimen cyclophosphamide + doxorubicin + cisplatin. Subgroup analysis revealed no group for which treatment assignment caused significant differences in either progression-free survival or overall survival. The study chairman reported that "even if there is (ultimately) a difference in survival, it will probably be only about 2%." Though there had been an initial suggestion (reported in the printed abstract) that patients with bulky disease benefited more from Taxol, this difference was not sustained in the longer-term data which was reported at the meeting. Note: The full results of the ICON3 trial have now been published (click here). Based on the clinical trials results showing no difference between single agent platinums (cisplatin or carboplatin) versus platinum/Taxol (GOG Trial # 132, ICON3), the British National Institute for Clinical Excellence (NICE) determined that platinum/Taxol should no longer be considered as "standard therapy" (click here for summary and click here for PDF file of document reviewing data and explaining recommendations) and that a range of therapies are equally acceptable. In the USA, where the administration of platinum/Taxol has been much more profitable to the treating oncologist than single agent platinum, there has been the dogged insistance that platinum/Taxol remains "standard," despite clear lack of support for this position, based on the entirety of the clinical trials literature.
Conclusions
I doubt that objective reviewers outside of the academic clinical
oncology
establishment would conclude that the paradigm of performing huge
randomized
studies to identify the best treatment to give to the average patient
has been productive with regard to identifying improved drug regimens.
At the end of the day, the only clear conclusion possible after
more than 20 years of these cooperative group trials of empiric
chemotherapy
in ovarian cancer is that there is no clear and meaningful advantage
associated
with any form of therapy ever examined in these trials.
What makes more sense?
1. Treat all patients with carboplatin/Taxol?
2. Choose between reasonable treatment regimens
(e.g. single agent carboplatin, carboplatin/Taxol, cisplatin/doxorubicin/cyclophosphamide,
gemcitabine/cisplatin, cisplatin/topotecan, cisplatin/vinorelbine,
cisplatin/Doxil,
cisplatin/etoposide, vinorelbine/Taxol, vinorelbine/docetaxel,
gemcitabine/vinorelbine,
vinorelbine/thiotepa, cyclophosphamide/doxorubicin, etc.) with the
assistance
of information from a well-validated Human Tumor Assay performed by an
experienced laboratory?
Larry M. Weisenthal
April 14, 2003
{kind=link}